Introduction: The Hidden Risk in Venous stents & Flow Diverters
Venous stents and neurovascular flow diverters are critical in managing conditions like chronic venous insufficiency and brain aneurysms. Yet, despite their benefits, a persistent challenge remains: blood-contacting surfaces that trigger thrombus formation. This risk compromises patient safety, prolongs recovery, and increases the need for intensive pharmacologic therapy. Hemocompatible coatings are essential—not optional—for mitigating these risks while supporting long-term healing.
Traditional drug-eluting coatings help prevent tissue regrowth but come at the cost of delayed healing and dependency on dual antiplatelet therapy. This creates a clinical dilemma, particularly in venous and neurovascular applications, where thrombosis—not restenosis—is the dominant cause of failure.
Camouflage™ by Smart Reactors offers a drug-free alternative engineered to support healing and long-term biocompatibility without compromising mechanical performance.
Understanding Venous Stents & Flow Diverters
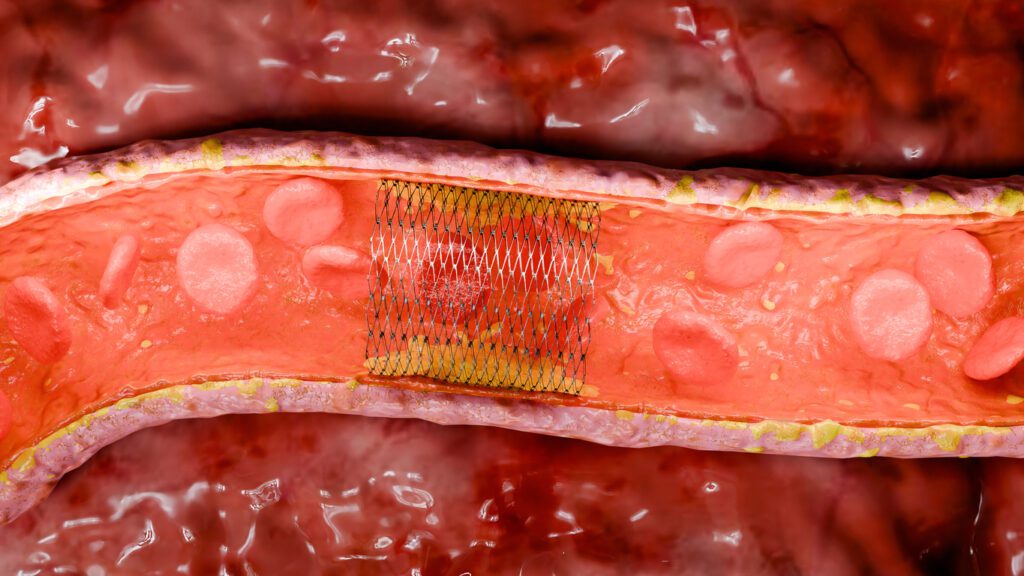
Venous stents are devices designed to support narrowed or collapsed veins and restore blood flow. Their applications range from deep vein thrombosis to post-thrombotic syndrome and iliofemoral obstruction. These stents must remain open long-term to maintain perfusion and prevent life-threatening complications such as pulmonary embolism.
Flow diverters, on the other hand, are cylindrical mesh implants used to treat complex or wide-neck brain aneurysms. Placed endovascularly, they redirect blood away from the aneurysm sac, inducing thrombosis within it and promoting vessel wall remodeling. Unlike coiling, which fills the aneurysm, flow diverters act externally—preserving the parent vessel’s integrity.
Complications That Undermine Device Success
Despite being life-saving, these devices carry significant risks:
- Thrombosis: Contact between blood and foreign material can activate the coagulation cascade, leading to clot formation that may block the vessel or embolize downstream.
- Delayed endothelialization: A surface that does not support endothelial growth can prolong exposure to clotting risk and increase device failure.
- Restenosis: While more common in arterial systems, vessel re-narrowing from hyperplasia can affect long-term patency.
- Drug dependence: Long-term use of antiplatelet therapy adds complexity and bleeding risk, particularly in patients with comorbidities or compliance issues.
Drug-eluting coatings release medication to control cell proliferation but often delay re-endothelialization. Over time, the drug reservoir depletes—reducing effectiveness and leaving the surface exposed. These trade-offs are especially problematic in non-arterial systems where the risk of thrombosis is higher than that of restenosis.
Procedure For Stent & Flow Diverter Placement
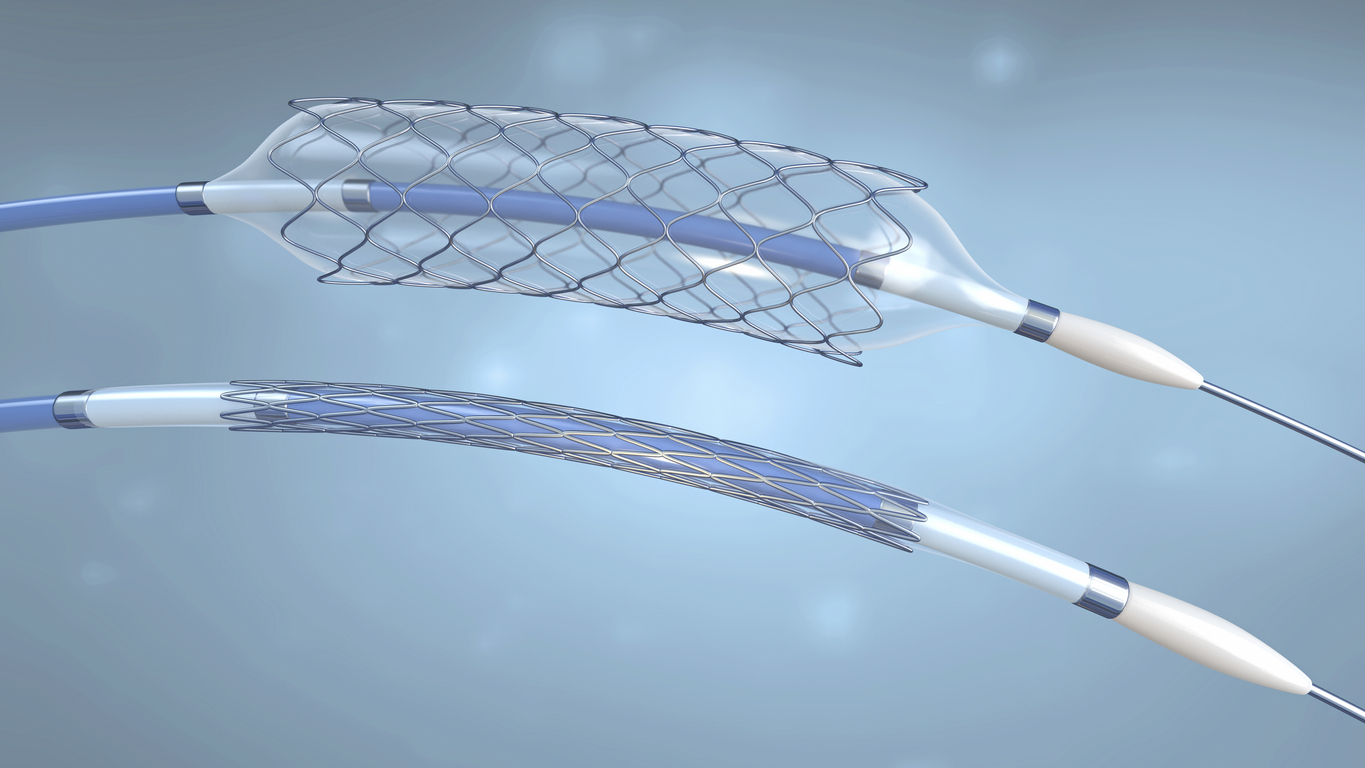
The procedure involved in placing a stent or flow diverter is minimally invasive compared to surgical alternatives. In preparation, the patient receives a general or local anesthetic depending on the type of procedure being carried out. A thin, flexible tube known as a catheter is placed into a large artery in the groin or arm to allow for the stent or flow diverter to be inserted.
Using fluoroscopy, the device is then guided to the desired location. Prior to this procedure, the stent is crimped to reduce the size of the device to allow ease of access through the patient’s vascular system. When the stent is positioned in the desired location, a small ballon is used to expand the stent allowing it to support and open the affected vessels. Alternatively, a self-expanding stent can be used which doesn’t require a balloon catheter.
Post-procedure patients may need to remain in the hospital for observation, though the duration of stay is typically much shorter compared to more invasive surgeries. In many cases, patients utilize a combination of dual antiplatelet therapy and blood filters, working synergistically to effectively prevent thrombus formation. Concerns regarding patient adherence to such medication are the primary driving forces for the use of hemocompatible coating technologies on such devices to reduce the risk of thrombus formation.
Common Materials Used In Stent & Flow Diverter Manufacturing
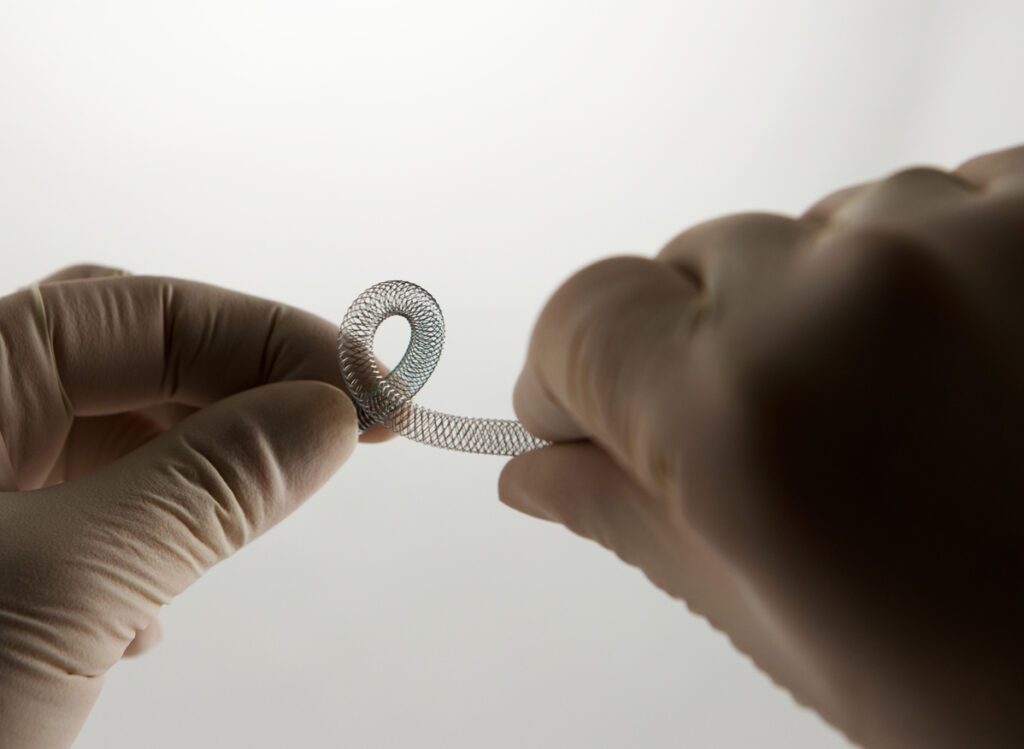
Stents and flow diverters can be made from a variety of materials including metal alloys, polymers, or a combination of materials. Generally, nitinol and cobalt chromium are the primary materials used when fabricating stents and flow diverters.
Nitinol is a metal alloy composed of equal parts nickel and titanium. This material is used in the field of medical devices due to its super elastic properties making it up to 10 times more flexible than other metals as well as its thermal shape memory properties. This shape memory effect describes a metal that can undergo a reversible phase transformation between Austenite and Martensite. Under high temperatures, nitinol enters the Austenite phase. In this phase, it achieves maximum stiffness and is spring-like when bent. During low temperatures, nitinol enters the Martensite phase. In this phase, the metal feels rubbery and bends easily.
In its Martensite state, nitinol can be easily set into a new shape. However, when heated through its transformation temperature, it reverts to Austenite and returns to its previous shape.
Slight changes in the alloy composition or heat treatment affect the temperature at which nitinol remembers its high-temperature form.
The specific application for the device determines the optimal transition temperature. In the case of stents, a transition temperature close to or equal to human body temperature is selected allowing the stent to revert to its original shape post crimping.
Cobalt chromium is another commonly used material for stents but is mainly used in flow diverter manufacturing. This is due to its high corrosion resistance and biocompatibility which reduces complications with surrounding tissue when implanted. Additionally, it is a chemically inert material that can minimize the possibility of irritation, allergic reaction, and immune response. Cobalt chromium is also an extremely strong alloy allowing for thinner struts while maintaining radial strength.
Selection of Stent Materials: The Importance of Hemocompatible Coatings
There are a variety of risks associated with stents and flow diverters including stent restenosis, which is the narrowing of the stent area after treatment (in arterial vessels), and the risk of blood clot formation. While the materials used for stents and flow diverters have a natural level of biocompatibility, it is insufficient to prevent thrombus formation and thus risking health complications for the patient. It is recommended that blood thinning medication is taken to minimize the initiation of the blood clotting cascade.
Restenosis is the most common clinical complication associated with arterial stents. Drug-eluting coatings are used to reduce potential restenosis. However, venous stents or neurovascular flow diverters carry a higher risk of thrombosis.
Drug-eluting stents help to prevent restenosis by using a thin coating that delivers medication directly to the bloodstream and the arterial walls. This inhibits cell proliferation to mitigate cell growth through the spaces between struts. Consequently, this disrupts endothelization of the stent surface and re-endothelization of the vessel walls. The resulting consequence is the delay in the healing process of the vessel wall as well as preventing long-term hemocompatibility and the risk of thrombus formation further down the line. There are also a variety of complications associated with long-term exposure to the medications used in drug-eluting stents. Drug-eluting coatings are not considered a desirable solution in the venous or neurovascular system as restenosis is not the major cause of clinical failure. Drug-eluting coatings gradually deplete their drug supply over time, which can lead to the re-emergence of complications as the coating loses its therapeutic effect.
Why Camouflage™ Is a Superior Hemocompatible Coating
Smart Reactors’ Camouflage™ coating offers:
- Excellent resistance to thrombus formation
- Compatibility with high-pressure crimping and self-expansion
- Stable under high shear rates seen in cerebral vasculature
- Promotes endothelialization across complex geometries
- Free from pharmaceutical agents, removing risks tied to long-term drug exposure
Camouflage™ is engineered with ultra-thin film deposition technology that ensures uniform coverage without blocking stent struts or changing flow profiles.
Testing and Validation
1. Chandler Loop System
- Mimics physiological blood flow
- Measures biomarkers post-circulation to evaluate thrombotic potential
- Camouflage™ has shown marked reductions in thrombin generation, platelet adhesion, and complement activation compared to uncoated controls
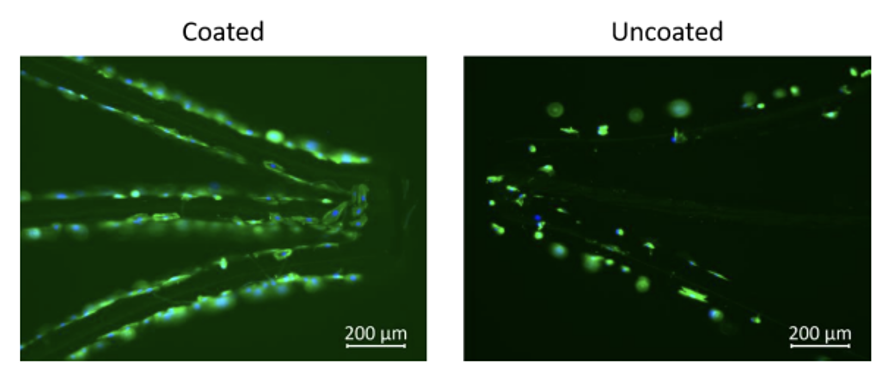
2. Cell Culture Assays
- Coated devices are incubated with HUVECs (Human Umbilical Vein Endothelial Cells)
- Fluorescence microscopy assesses adhesion and growth
- Cytotoxicity assays confirm viability and healthy morphology of adhered cells
- Camouflage™ supports confluent monolayer formation, a key indicator of vessel wall integration
Conclusion
Stents and Flow Diverters are crucial in the medical device industry providing lifesaving treatment with minimally invasive procedures. Stents help support weakened or blocked blood vessels while flow diverters are crucial in the management of complex brain aneurysms. However, with all blood-contacting medical devices, there is a risk of thrombus formation due to poor material hemocompatibility. This highlights the vital importance of hemocompatible coatings such as Smart Reactors Camouflage™ to help reduce the risk of blood clot formation improving the long-term hemocompatibility of Stents and Flow Diverters.
Current Publications